What is a fistula?
 The word Fistula means a pipe, tube. Fistula defined as an abnormal passage between interior of the anal canal [or rectum] and the outer skin surface around the anus; A fistula, therefore, consists of –
The word Fistula means a pipe, tube. Fistula defined as an abnormal passage between interior of the anal canal [or rectum] and the outer skin surface around the anus; A fistula, therefore, consists of –
- The internal opening which is inside the anus or rectum,
- The external opening which is on the skin surface around the anus,
- A tube-like structure that connects internal and external opening.
What are the types of fistula ?
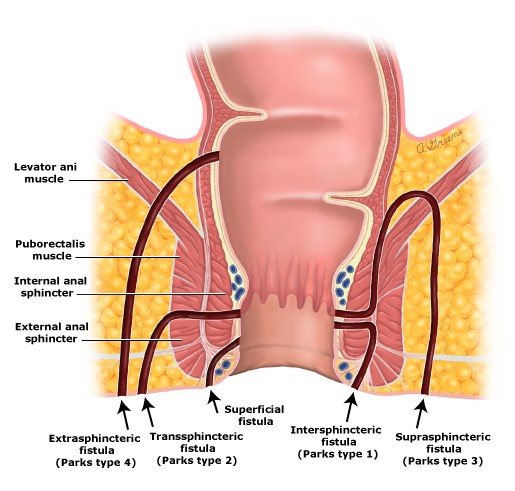
Based on pathogenesis & course of anal fistulae in relation to external sphincter fistulas are classified into the following types
- Intersphincteric
- Transphincteric
- Suprasphincteric
- Extrasphincteric
However for all clinical purposes fistulas are widely divided into:
- Simple fistula
- Complex fistula
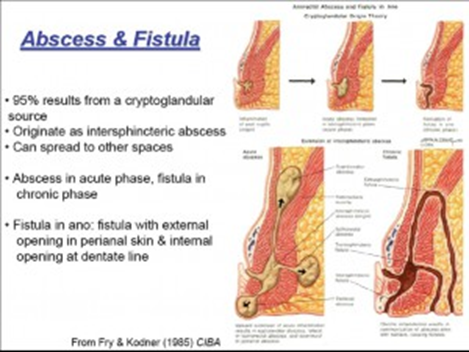
 What are the symptoms of an abscess?
What are the symptoms of an abscess?
- Ano-rectal pain
- Swelling and fluctuance
- Drainage of pus and blood
- Fever
- Irritation of skin
- Itching
 Most of these procedures mentioned above do not or minimally damage the sphincter but have a cure rate of around 40 to 70% depending upon the procedures. Some of these procedures like Plug, VAAFT, Cell Therapy, LASER are very costly too thereby limiting their use.
Most of these procedures mentioned above do not or minimally damage the sphincter but have a cure rate of around 40 to 70% depending upon the procedures. Some of these procedures like Plug, VAAFT, Cell Therapy, LASER are very costly too thereby limiting their use.
The choice of the procedure for a particular type of fistula is always decided by the surgeon depending upon the complexity of the disease and his personal training and experience in dealing with the same.
Complications of fi stula
stula
- Recurrence of disease – this is very common in fistula cases and must be understood by the patient before undergoing the same. For simple fistula, the recurrence rate is around 5% if fistulotomy or fistulectomy is done. However, with complex fistula the recurrence rate is almost up to 30 % of cases depending upon the procedure adopted. The least recurrent cases are found with primary sphincter repair surgery.
- Incontinence – that is the loss of control of the passage of stools. The degree varies from minor incontinences which could be just urgency for passing stools and inability to control gases and at times liquid stool especially in diarrhoea to major incontinence such as complete inability to control even solid stools. The sphincter sparing procedure described above causes the least incontinence whereas the others have a varying degree of minor to major incontinences rates.
- The other complication includes bleeding, urinary retention, constipation, delayed healing of the wounds

What will be the duration of hospital stay?
Depending upon the fistula tract and procedure done hospital stay may vary from 1 day to 3 days depending upon the type of fistula and the procedure undertaken along with the general condition of the patient.
Anaesthesia used –
Depending upon the surgeon and the anaesthetist choice, some form of regional anaesthesia like spinal, saddle are used. Some use general anaesthesia. Few opt for local anaesthesia with sedation.
How to take care of the post-operative wound?
The dressing will be done daily by the doctor for some days after the operation and later patient or relative will be educated to do the dressing at home and will be asked to visit the doctor after 2 days or once in a week to assess the wound if any changes are required or not. The patient will be advised daily sitz bath at least 3 times a day. The dressing needs to be done after passage of every stool so that no faecal contamination remains.
Re-joining the Work:
The amount of time you will be off work after surgery depends on both your surgery and your job. This should have been discussed with your doctor before surgery. Most patients are however able to join within a week time to 10 days. The others who can work from home as early as their discharge
Now you have Laser Surgery option too. Please see below image to view the details.